
Chronic Obstructive Pulmonary Disease (COPD)
 |
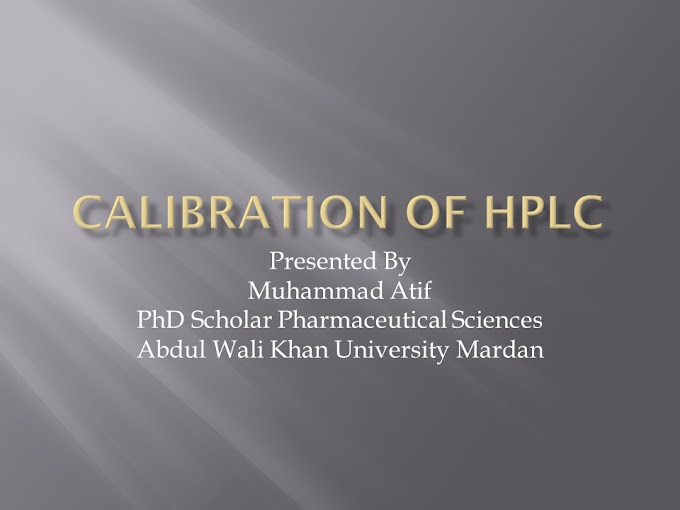
| Healthy lungs have open airways versus the collapsed and narrow airways of emphysema and bronchitis, conditions grouped under COPD. |
OverviewChronic obstructive pulmonary disease (COPD)Chronic obstructive pulmonary disease (COPD) is the name for a group of lung conditions that cause breathing difficulties.
It includes:
- emphysema – damage to the air sacs in the lungs
- chronic bronchitis – long-term inflammation of the airways
COPD is a common condition that mainly affects middle-aged or older adults who smoke. Many people do not realise they have it.
The breathing problems tend to get gradually worse over time and can limit your normal activities, although treatment can help keep the condition under control.
Chronic obstructive pulmonary disease (COPD) is the name for a group of lung conditions that cause breathing difficulties.
It includes:
- emphysema – damage to the air sacs in the lungs
- chronic bronchitis – long-term inflammation of the airways
COPD is a common condition that mainly affects middle-aged or older adults who smoke. Many people do not realise they have it.
The breathing problems tend to get gradually worse over time and can limit your normal activities, although treatment can help keep the condition under control.
Symptoms of COPD
The main symptoms of COPD are:
- increasing breathlessness, particularly when you're active
- a persistent chesty cough with phlegm – some people may dismiss this as just a "smoker's cough"
- frequent chest infections
- persistent wheezing
Without treatment, the symptoms usually get progressively worse. There may also be periods when they get suddenly worse, known as a flare-up or exacerbation.
Read also:
The main symptoms of COPD are:
- increasing breathlessness, particularly when you're active
- a persistent chesty cough with phlegm – some people may dismiss this as just a "smoker's cough"
- frequent chest infections
- persistent wheezing
Without treatment, the symptoms usually get progressively worse. There may also be periods when they get suddenly worse, known as a flare-up or exacerbation.
Read also:
When to get medical advice
See a General Physician if you have persistent symptoms of COPD, particularly if you're over 35 and smoke or used to smoke.
Do not ignore the symptoms. If they're caused by COPD, it's best to start treatment as soon as possible, before your lungs become significantly damaged.
The GP will ask about your symptoms and whether you smoke or have smoked in the past. They can organise a breathing test to help diagnose COPD and rule out other lung conditions, such as asthma.
See a General Physician if you have persistent symptoms of COPD, particularly if you're over 35 and smoke or used to smoke.
Do not ignore the symptoms. If they're caused by COPD, it's best to start treatment as soon as possible, before your lungs become significantly damaged.
The GP will ask about your symptoms and whether you smoke or have smoked in the past. They can organise a breathing test to help diagnose COPD and rule out other lung conditions, such as asthma.
Causes of COPD
COPD happens when the lungs become inflamed, damaged and narrowed. The main cause is smoking, although the condition can sometimes affect people who have never smoked.
The likelihood of developing COPD increases the more you smoke and the longer you've smoked.
Some cases of COPD are caused by long-term exposure to harmful fumes or dust. Others are the result of a rare genetic problem which means the lungs are more vulnerable to damage.
COPD happens when the lungs become inflamed, damaged and narrowed. The main cause is smoking, although the condition can sometimes affect people who have never smoked.
The likelihood of developing COPD increases the more you smoke and the longer you've smoked.
Some cases of COPD are caused by long-term exposure to harmful fumes or dust. Others are the result of a rare genetic problem which means the lungs are more vulnerable to damage.
Treatments for COPD
The damage to the lungs caused by COPD is permanent, but treatment can help slow down the progression of the condition.
Treatments include:
- stopping smoking – if you have COPD and you smoke, this is the most important thing you can do
- inhalers and medicines – to help make breathing easier
- pulmonary rehabilitation – a specialised programme of exercise and education
- surgery or a lung transplant – although this is only an option for a very small number of people
The damage to the lungs caused by COPD is permanent, but treatment can help slow down the progression of the condition.
Treatments include:
- stopping smoking – if you have COPD and you smoke, this is the most important thing you can do
- inhalers and medicines – to help make breathing easier
- pulmonary rehabilitation – a specialised programme of exercise and education
- surgery or a lung transplant – although this is only an option for a very small number of people
Outlook for COPD
The outlook for COPD varies from person to person. The condition cannot be cured or reversed, but for many people, treatment can help keep it under control so it does not severely limit their daily activities.
But in some people, COPD may continue to get worse despite treatment, eventually having a significant impact on their quality of life and leading to life-threatening problems.
The outlook for COPD varies from person to person. The condition cannot be cured or reversed, but for many people, treatment can help keep it under control so it does not severely limit their daily activities.
But in some people, COPD may continue to get worse despite treatment, eventually having a significant impact on their quality of life and leading to life-threatening problems.
Social care and support guide
If you:
- need help with day-to-day living because of illness or disability
- care for someone regularly because they're ill, elderly or disabled – including family members
If you:
- need help with day-to-day living because of illness or disability
- care for someone regularly because they're ill, elderly or disabled – including family members
Preventing COPD
COPD is largely a preventable condition. You can significantly reduce your chances of developing it if you avoid smoking.
If you already smoke, stopping can help prevent further damage to your lungs before it starts to cause troublesome symptoms.
COPD is largely a preventable condition. You can significantly reduce your chances of developing it if you avoid smoking.
If you already smoke, stopping can help prevent further damage to your lungs before it starts to cause troublesome symptoms.
Symptoms
Chronic obstructive pulmonary disease (COPD) makes breathing increasingly more difficult. But it develops slowly over many years and you may not be aware you have it at first.
Most people with COPD do not have any noticeable symptoms until they reach their late 40s or 50s.
Main symptoms
Common symptoms of COPD include:
- increasing breathlessness – this may only happen when exercising at first, and you may sometimes wake up at night feeling breathless
- a persistent chesty cough with phlegm that does not go away
- frequent chest infections
- persistent wheezing
The symptoms will usually get gradually worse over time and make daily activities increasingly difficult, although treatment can help slow the progression.
Sometimes there may be periods when your symptoms get suddenly worse – known as a flare-up or exacerbation. It's common to have a few flare-ups a year, particularly during the winter.
If you have a high temperature or you do not feel well enough to do your normal activities, try to stay at home and avoid contact with other people until you feel better.
Other symptoms
Less common symptoms of COPD include:
- weight loss
- tiredness
- swollen ankles from a build-up of fluid (oedema)
- chest pain and coughing up blood – although these are usually signs of another condition, such as a chest infection or possibly lung cancer
These additional symptoms only tend to happen when COPD reaches an advanced stage.
When to get medical advice
See a GP if you have persistent symptoms of COPD, particularly if you're over 35 and smoke or used to smoke.
There are several conditions that cause similar symptoms, such as asthma, bronchiectasis, anaemia and heart failure. A simple breathing test can help determine if you have COPD.
While there's currently no cure for COPD, the sooner treatment begins, the less chance there is of severe lung damage.
Read also:
- Dengue awareness
- How To Treat Low Blood Sugar (Hypoglycemia)
- Eye Disorders and Diseases
- Heart Attack Symptoms, Risk, and Recovery
- Heart Failure
- ANTIRHEUMATIC DRUGS
- Diabetes and types of Diabetes
- High Blood Pressure Symptoms and Causes
Causes
Chronic obstructive pulmonary disease (COPD) happens when the lungs and airways become damaged and inflamed.
It's usually associated with long-term exposure to harmful substances such as cigarette smoke.
Things that can increase your risk of developing COPD are discussed in this section.
Smoking
Smoking is the main cause of COPD and is thought to be responsible for around 9 in every 10 cases.
The harmful chemicals in smoke can damage the lining of the lungs and airways. Stopping smoking can help prevent COPD from getting worse.
Some research also suggests that being exposed to other people's cigarette smoke (passive smoking) may increase your risk of COPD.
Fumes and dust at work
Exposure to certain types of dust and chemicals at work may damage the lungs and increase your risk of COPD.
Substances that have been linked to COPD include:
- cadmium dust and fumes
- grain and flour dust
- silica dust
- welding fumes
- isocyanates
- coal dust
The risk of COPD is even higher if you breathe in dust or fumes in the workplace and you smoke.
Air pollution
Exposure to air pollution over a long period can affect how well the lungs work and some research suggests it could increase your risk of COPD.
But at the moment the link between air pollution and COPD is not conclusive and research is continuing.
Genetics
You're more likely to develop COPD if you smoke and have a close relative with the condition, which suggests some people's genes might make them more vulnerable to the condition.
Around 1 in 100 people with COPD has a genetic tendency to develop the condition, called alpha-1-antitrypsin deficiency. Alpha-1-antitrypsin is a substance that protects your lungs. Without it, the lungs are more vulnerable to damage.
People who have an alpha-1-antitrypsin deficiency usually develop COPD at a younger age – particularly if they smoke.
The British Lung Foundation has more information about alpha-1-antitrypsin deficiency.
There are also 2 charities for people affected by alpha-1-antitrypsin deficiency:
Diagnosis
See a General Physician if you have persistent symptoms of chronic obstructive pulmonary disease (COPD).
To help them diagnose COPD, a General Physician may:
- ask you about your symptoms
- examine your chest and listen to your breathing using a stethoscope
- ask whether you smoke or used to smoke
- calculate your body mass index (BMI) using your weight and height
- ask if you have a family history of lung problems
They may also do, or arrange for you to have, a breathing test called spirometry, plus other related tests of the lungs and airways.
Spirometry
A test called spirometry can help show how well your lungs are working.
You'll be asked to breathe into a machine called a spirometer after inhaling a medicine called a bronchodilator, which helps widen your airways.
The spirometer takes 2 measurements: the volume of air you can breathe out in a second, and the total amount of air you breathe out. You may be asked to breathe out a few times to get a consistent reading.
The readings are compared with normal results for your age, which can show if your airways are obstructed.
Chest X-ray
A chest X-ray can be used to look for problems in the lungs that can cause similar symptoms to COPD.
Problems that can be shown by an X-ray include chest infections and lung cancer, although these do not always show.
Blood tests
A blood test can show other conditions that can cause similar symptoms to COPD, such as a low iron level (anaemia) and a high concentration of red blood cells in your blood (polycythaemia).
Sometimes a blood test may also be done to see if you have alpha-1-antitrypsin deficiency. This is a rare genetic problem that increases your risk of COPD.
Further tests
Sometimes more tests may be needed to confirm the diagnosis or determine the severity of your COPD.
This will help you and your doctor plan your treatment.
These tests may include:
- an electrocardiogram (ECG) – a test that measures the electrical activity of the heart
- an echocardiogram – an ultrasound scan of the heart
- a peak flow test – a breathing test that measures how fast you can blow air out of your lungs, which can help rule out asthma
- a blood oxygen test – a peg-like device is attached to your finger to measure the level of oxygen in your blood
- a CT scan – a detailed scan that can help identify any problems in your lungs
- a phlegm sample – a sample of your phlegm (sputum) may be tested to check for signs of a chest infection
Read also:
- Dengue awareness
- How To Treat Low Blood Sugar (Hypoglycemia)
- Eye Disorders and Diseases
- Heart Attack Symptoms, Risk, and Recovery
- Heart Failure
- ANTIRHEUMATIC DRUGS
- Diabetes and types of Diabetes
- High Blood Pressure Symptoms and Causes
Treatment
There's currently no cure for chronic obstructive pulmonary disease (COPD), but treatment can help slow the progression of the condition and control the symptoms.
Treatments include:
- stopping smoking – if you have COPD and you smoke, this is the most important thing you can do
- inhalers and tablets – to help make breathing easier
- pulmonary rehabilitation – a specialised programme of exercise and education
- surgery or a lung transplant – although this is only an option for a very small number of people
A doctor will discuss the various treatment options with you.
Stop smoking
If you smoke, stopping is the most effective way to prevent COPD getting worse.
Although any damage done to your lungs and airways cannot be reversed, giving up smoking can help prevent further damage.
This may be all the treatment that's needed in the early stages of COPD, but it's never too late to stop – even people with more advanced COPD will benefit from quitting.
Inhalers
If COPD is affecting your breathing, you'll usually be given an inhaler. This is a device that delivers medicine directly into your lungs as you breathe in.
A doctor or nurse will advise you on how to use an inhaler correctly and how often to use it.
There are several different types of inhaler for COPD. The main types include:
Short-acting bronchodilator inhalers
For most people with COPD, short-acting bronchodilator inhalers are the first treatment used.
Bronchodilators are medicines that make breathing easier by relaxing and widening your airways.
There are 2 types of short-acting bronchodilator inhaler:
- beta-2 agonist inhalers – such as salbutamol and terbutaline
- antimuscarinic inhalers – such as ipratropium
Short-acting inhalers should be used when you feel breathless, up to a maximum of 4 times a day.
Long-acting bronchodilator inhalers
If you experience symptoms regularly throughout the day, a long-acting bronchodilator inhaler will be recommended.
These work in a similar way to short-acting bronchodilators, but each dose lasts for at least 12 hours, so they only need to be used once or twice a day.
There are 2 types of long-acting bronchodilator inhaler:
- beta-2 agonist inhalers – such as salmeterol, formoterol and indacaterol
- antimuscarinic inhalers – such as tiotropium, glycopyronium and aclidinium
Some new inhalers contain a combination of a long-acting beta-2 agonist and antimuscarinic.
Steroid inhalers
If you're still becoming breathless when using a long-acting inhaler, or you have frequent flare-ups (exacerbations), a GP may suggest including a steroid inhaler as part of your treatment.
Steroid inhalers contain corticosteroid medicines, which can help to reduce the inflammation in your airways.
Steroid inhalers are normally prescribed as part of a combination inhaler that also includes a long-acting medicine.
Tablets
If your symptoms are not controlled with inhalers, a doctor may recommend taking tablets or capsules as well.
Theophylline tablets
Theophylline is a type of bronchodilator. It's unclear exactly how theophylline works, but it seems to reduce swelling (inflammation) in the airways and relax the muscles lining them.
Theophylline comes as tablets or capsules and is usually taken twice a day.
You may need to have regular blood tests during treatment to check the level of medicine in your blood.
This will help a doctor work out the best dose to control your symptoms while reducing the risk of side effects.
Possible side effects include:
- feeling and being sick
- headaches
- difficulty sleeping (insomnia)
- noticeable pounding, fluttering or irregular heartbeats (palpitations)
Sometimes a similar medicine called aminophylline is also used.
Mucolytics
If you have a persistent chesty cough with lots of thick phlegm, the doctor may recommend taking a mucolytic medicine called carbocisteine.
Mucolytic medicines make the phlegm in your throat thinner and easier to cough up.
Carbocisteine comes as tablets or capsules and is usually taken 3 or 4 times a day.
If carbocisteine does not help your symptoms, or you cannot take it for medical reasons, another mucolytic medicine called acetylcysteine is available.
This comes as a powder that you mix with water. Acetylcysteine powder has an unpleasant smell, like rotten eggs, but this smell should go away once you mix it with the water.
Steroid tablets
If you have a particularly bad flare-up, you may be prescribed a short course of steroid tablets to reduce the inflammation in your airways.
A 5-day course of treatment is usually recommended, as long-term use of steroid tablets can cause troublesome side effects such as:
- weight gain
- mood swings
- weakened bones (osteoporosis)
Your doctor may give you a supply of steroid tablets to keep at home to take as soon as you experience a bad flare-up.
Longer courses of steroid tablets must be prescribed by a COPD specialist. You'll be given the lowest effective dose and monitored closely for side effects.
Antibiotics
Your doctor may prescribe a short course of antibiotics if you have signs of a chest infection, such as:
- becoming more breathless
- coughing more
- noticing a change in the colour (such as becoming brown, green or yellow) and/or consistency of your phlegm (such as becoming thicker)
Sometimes you may be given a course of antibiotics to keep at home and take as soon as you experience symptoms of an infection.
Pulmonary rehabilitation
Pulmonary rehabilitation is a specialised programme of exercise and education designed to help people with lung problems such as COPD.
It can help improve how much exercise you're able to do before you feel out of breath, as well as your symptoms, self-confidence and emotional wellbeing.
Pulmonary rehabilitation programmes usually involve 2 or more group sessions a week for at least 6 weeks.
A typical programme includes:
- physical exercise training tailored to your needs and ability – such as walking, cycling and strength exercises
- education about your condition for you and your family
- dietary advice
- psychological and emotional support
The programmes are provided by a number of different healthcare professionals, including physiotherapists, nurse specialists and dietitians.
Improving muscle strength
If you are having a bad flare-up and are unable to exercise, you may be offered electrical stimulation to make your muscles stronger.
This is where electrodes are placed on your skin and small electrical impulses are sent to weak muscles, usually in your arms or legs.
Other treatments
If you have severe symptoms or experience a particularly bad flare-up, you may sometimes need additional treatment.
Nebulised medicine
Nebulised medicine may be used in severe cases of COPD if inhalers have not worked.
This is where a machine is used to turn liquid medicine into a fine mist that you breathe in through a mouthpiece or a face mask. It enables a large dose of medicine to be taken in one go.
You'll usually be given a nebuliser device to use at home after being shown how to use it.
Roflumilast
Roflumilast is a new medicine that can be used to treat flare-ups.
It is recommended for people whose symptoms have suddenly become worse at least 2 times over the past 12 months, and who are already using inhalers.
Roflumilast comes as tablets and the medicine helps reduce inflammation inside the lungs and airways.
Side effects of roflumilast include:
- feeling and being sick
- diarrhoea
- reduced appetite
- weight loss
- headache
Long-term oxygen therapy
If COPD causes a low level of oxygen in your blood, you may be advised to have oxygen at home through nasal tubes or a mask.
This can help stop the level of oxygen in your blood becoming dangerously low, although it's not a treatment for the main symptoms of COPD, such as breathlessness.
Long-term oxygen treatment should be used for at least 16 hours a day.
The tubes from the machine are long, so you will be able to move around your home while you're connected. Portable oxygen tanks are available if you need to use oxygen away from home.
Do not smoke when using oxygen. The increased level of oxygen is highly flammable and a lit cigarette could cause a fire or explosion.
Ambulatory oxygen therapy
Some people with COPD will benefit from ambulatory oxygen, which is oxygen you use when you walk or are active in other ways.
If your blood oxygen levels are normal while you're resting but fall when you exercise, you may be able to have ambulatory oxygen therapy rather than long-term oxygen therapy.
Non-invasive ventilation (NIV)
If you're taken to hospital because of a bad flare-up, you may have a treatment called non-invasive ventilation (NIV).
This is where a portable machine connected to a mask that covers your nose or face is used to support your lungs and make breathing easier.
Surgery
Surgery is usually only suitable for a small number of people with severe COPD whose symptoms are not controlled with medicine.
There are 3 main operations that can be done:
- bullectomy – an operation to remove a pocket of air from one of the lungs, allowing the lungs to work better and make breathing more comfortable
- lung volume reduction surgery – an operation to remove a badly damaged section of lung to allow the healthier parts to work better and make breathing more comfortable
- lung transplant – an operation to remove and replace a damaged lung with a healthy lung from a donor.
Read also:
- Dengue awareness
- How To Treat Low Blood Sugar (Hypoglycemia)
- Eye Disorders and Diseases
- Heart Attack Symptoms, Risk, and Recovery
- Heart Failure
- ANTIRHEUMATIC DRUGS
- Diabetes and types of Diabetes
- High Blood Pressure Symptoms and Causes
Living with
Chronic obstructive pulmonary disease (COPD) can affect many aspects of your life. But there are some ways to help reduce its impact.
Looking after yourself
It's important to take good care of yourself if you have COPD.
Some of the main things you'll be advised to do are outlined below.
Take your medicine
It's important to take any prescribed medicine, including inhalers, as this can help prevent bad flare-ups.
It's also a good idea to read the information leaflet that comes with your medicine about possible interactions with other medicines or supplements.
Check with your care team if you plan to take any over-the-counter remedies, such as painkillers or nutritional supplements. These can sometimes interfere with your medicine.
Also speak to your care team if you have any concerns about the medicine you're taking or you're experiencing any side effects.
Stop smoking
If you smoke, stopping can help slow down or prevent further damage to your lungs.
Help is available from a GP and NHS stop smoking services.
Find about more about how to stop smoking.
Exercise regularly
Exercising regularly can help improve your symptoms and quality of life.
The amount of exercise you can do will depend on your individual circumstances. Exercising until you're a little breathless is not dangerous, but do not push yourself too far.
It's a good idea to speak to a GP for advice before starting a new exercise programme if your symptoms are severe or you have not exercised in a while.
You may be advised to participate in a pulmonary rehabilitation programme, which will include a structured exercise plan tailored to your needs and ability.
Maintain a healthy weight
Carrying extra weight can make breathlessness worse, so it's a good idea to lose weight through a combination of regular exercise and a healthy diet if you're overweight.
Some people with COPD find that they unintentionally lose weight. Eating foods that are high in protein and taking in enough calories is important to maintain a healthy weight.
You may see a dietitian as part of a pulmonary rehabilitation program if necessary.
Get vaccinated
COPD can put a significant strain on your body and mean you're more vulnerable to infections.
Everyone with COPD is encouraged to have the annual flu jab and the one-off pneumococcal vaccination.
You can get these vaccinations at your GP surgery or a local pharmacy that offers a vaccination service.
Check the weather
Cold spells and periods of hot weather and humidity can cause breathing problems if you have COPD.
It's a good idea to keep an eye on the weather forecast and make sure you have enough of your medicine to hand in case your symptoms get temporarily worse.
Watch what you breathe
There are certain things that should be avoided, if possible, to reduce COPD symptoms and the chances of a flare-up, including:
- dusty places
- fumes, such as car exhausts
- smoke
- air freshener sprays or plug-ins
- strong-smelling cleaning products (unless there's plenty of ventilation)
- hairspray
- perfume
Regular reviews and monitoring
You'll have regular contact with your care team to monitor your condition.
These appointments may involve:
- talking about your symptoms – such as whether they're affecting your normal activities or are getting worse
- talking about your medicine – including whether you think you might be experiencing any side effects
- tests to monitor your health
It's also a good opportunity to ask any questions you have or raise any other issues you'd like to discuss with your care team.
Breathing techniques
There are various breathing techniques that some people find helpful for breathlessness.
These include breathing control, which involves breathing gently using the least effort, with the shoulders supported. This can help when people with COPD feel short of breath.
Breathing techniques for people who are more active include:
- relaxed, slow, deep breathing
- breathing through pursed lips, as if whistling
- breathing out hard when doing an activity that needs a big effort
- paced breathing, using a rhythm in time with the activity, such as climbing stairs
If you have a chesty cough that produces a lot of phlegm, you may be taught a specific technique to help you clear your airways called the active cycle breathing technique.
Talk to others
If you have questions about your condition and treatment, your GP or nurse may be able to reassure you.
You may also find it helpful to talk to a trained counsellor or psychologist, or someone at a specialist helpline.
Relationships and sex
Having a long-term illness such as COPD can put a strain on any relationship.
Relationships with friends and family
Difficulty breathing and coughing can make you feel tired and depressed.
Your spouse, partner or carer may also have a lot of concerns about your health. It's important to talk about your worries together.
Being open about how you feel and what your family and friends can do to help may put them at ease. But do not feel shy about telling them that you need some time to yourself, if that's what you want.
Your sex life
As COPD progresses, the increasing breathlessness can make it difficult to take part in strenuous activities. The breathlessness may happen during sexual activity.
Talk to your partner and stay open-minded. Explore what you both like sexually. Simply touching, being touched and being close to someone helps a person feel loved and special.
Your doctor, nurse or physiotherapist may also be able to suggest ways to help manage breathlessness during sex.
Flying with COPD
If you have COPD and are planning to fly, go to your GP for a fitness-to-fly assessment. This involves checking your breathing using spirometry and measuring your oxygen levels.
Before travelling, remember to pack all your medicine, such as inhalers, in your hand luggage.
If you're using oxygen therapy, tell your travel operator and airline before you book your holiday, as you may need to get a medical form from your GP.
If you're using long-term oxygen therapy, you'll need to make sure you have an adequate oxygen supply for your flight as well as for your time away.
Airlines generally do not allow you to bring oxygen cylinders with you but may permit portable oxygen concentrator devices.
End of life care
COPD is a serious condition that can eventually reach a stage where it becomes life threatening.
Talking about this and planning your end of life care, also called palliative care, in advance can be helpful.
It can be difficult to talk about dying with your doctor, and particularly with family and friends, but many people find it helps. Support is also available for your family and friends.
It may be helpful to discuss the symptoms you may have as you become more seriously ill, and the treatments available to manage these.
As COPD progresses, your doctor should work with you to establish a clear management plan based on your wishes. This will include whether you would prefer to go to hospital or a hospice, or be looked after at home as you become more ill.
Read also:



){kind=link}
0 Comments